From Wear-and-Tear to Regeneration: Can We Grow Back Knee Cartilage?
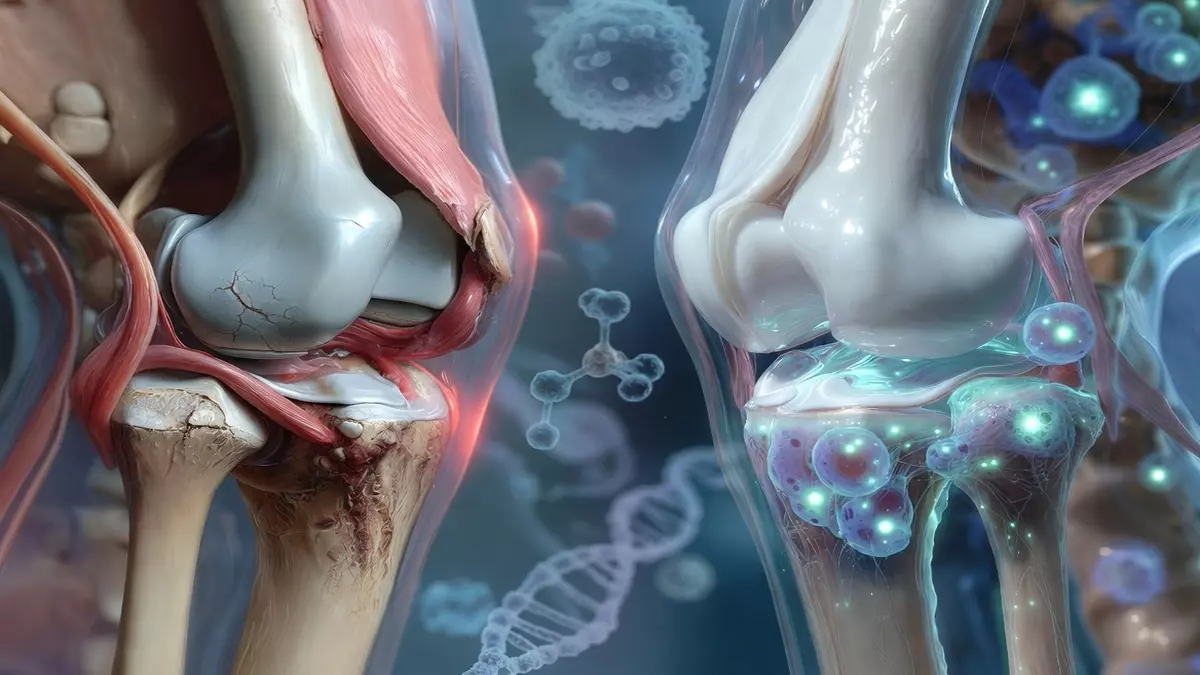
For millions of people, the daily routine of climbing stairs or rising from a chair is marked by the persistent ache of osteoarthritis. For decades, the medical community has viewed this condition as an inevitable “wear-and-tear” process—a one-way street of cartilage degradation that usually ends in pain management or invasive joint replacement surgery.
However, groundbreaking research from Stanford University is challenging this long-held narrative. Scientists have identified a specific protein that appears to act as an “aging switch” for joints. By blocking this protein, researchers have successfully stimulated the regrowth of cartilage in older mice, offering a tantalizing glimpse into a future where damaged joints might be repaired rather than replaced.
From Wear-and-Tear to Regeneration Can We Grow Back Knee Cartilage
The Role of 15-PGDH: An “Aging Switch” in Joints
The research, published in the journal Science, centers on a protein known as 15-PGDH. As we age, levels of this protein naturally increase within the body, interfering with the chemical signals responsible for tissue repair and inflammation control.

Stanford researchers hypothesized that this buildup of 15-PGDH is a primary driver of the joint degradation seen in osteoarthritis. To test this, they utilized a small-molecule inhibitor—a compound designed to block the protein’s activity. The results were striking: when the inhibitor was administered to older mice, their cartilage, which had thinned significantly due to age, began to thicken and regain its structural integrity.
Beyond Stem Cells: Retraining Existing Tissue
One of the most innovative aspects of this study is the method of regeneration. Historically, many attempts to heal cartilage have relied on stem cell therapy, which involves introducing new cells into the body to grow tissue.
This study suggests a different, more efficient path. Instead of importing external cells, the 15-PGDH inhibitor appears to “retrain” existing chondrocytes—the cells responsible for maintaining cartilage—causing them to revert to a more youthful, healthier state.

“This is a new way of regenerating adult tissue, and it has significant clinical promise for treating arthritis due to aging or injury,” said microbiologist Helen Blau of Stanford University. “We were looking for stem cells, but they are clearly not involved. It’s very exciting.”
Promising Results for Mobility and Human Tissue
The success in the laboratory extended to physical outcomes. Treated mice with knee injuries similar to an ACL tear showed:
Restored Mobility: Treated animals walked more steadily and applied more weight to their injured legs, indicating a significant reduction in pain.
Structural Repair: Cartilage thickness increased in the affected joints.
Human Tissue Compatibility: In laboratory tests using cartilage samples from patients undergoing knee replacement surgery, the inhibitor successfully pushed the tissue toward a more functional, less inflamed state.

While a lab sample is not a living joint, these findings provide a strong foundation for future clinical trials.
A Growing Shift in Osteoarthritis Research
This discovery arrives alongside other major shifts in how we understand and treat arthritis. The medical field is rapidly moving away from the simplistic “wear-and-tear” model:
Metabolic Influence: A February 2026 study published in Cell Metabolism highlighted that drugs like semaglutide may offer joint protection by targeting metabolic pathways inside the joint, independent of weight loss.
Advanced Delivery Systems: Engineers, such as those at the University of Colorado Boulder, are developing slow-release, injectable drug delivery systems designed to target damaged areas of the joint with higher precision.
These advancements suggest that osteoarthritis is far more “active” and treatable than previously assumed, potentially involving cellular and metabolic processes that can be influenced by medicine.
What This Means for the Future
Is a “cartilage-regrowth injection” hitting the market next week? Not quite. Translating success in mice to a safe, effective human therapy is a complex process. However, there is cause for optimism: the researchers noted that a 15-PGDH inhibitor has already cleared Phase 1 safety trials for muscle weakness, meaning significant safety data for humans already exists.
For now, this research changes the fundamental conversation around joint health. Instead of merely managing pain while waiting for the inevitable need for surgery, the scientific focus is moving toward genuine tissue restoration. It offers the hope that the “stiff mornings” of millions could eventually be a thing of the past.
Frequently Asked Questions (FAQ)
1. Is this a cure for arthritis?
While not yet a cure, this research represents a major breakthrough. It demonstrates that cartilage is capable of regeneration when specific molecular “brakes”—like the 15-PGDH protein—are removed.
2. When will this treatment be available to patients?
The research is currently in the experimental stage. While results in mice and human lab samples are promising, the next step will involve rigorous human clinical trials to ensure the treatment is safe and effective for long-term use in living joints.
3. How does this differ from stem cell therapy?
Stem cell therapy attempts to regrow tissue by introducing new, undifferentiated cells into the body. This new method works by “retraining” the body’s existing chondrocytes to repair the damage themselves.
4. Can this help with all types of joint pain?
The study specifically targeted osteoarthritis. While the mechanisms of cartilage health may overlap with other conditions, this specific research is focused on the age-related breakdown of joint cushioning.
5. Why is cartilage so hard to heal?
Cartilage is notoriously stubborn because it lacks a robust blood supply, which is necessary for the body to deliver the nutrients and cells needed for repair. This new method provides a way to stimulate repair from within the tissue itself.